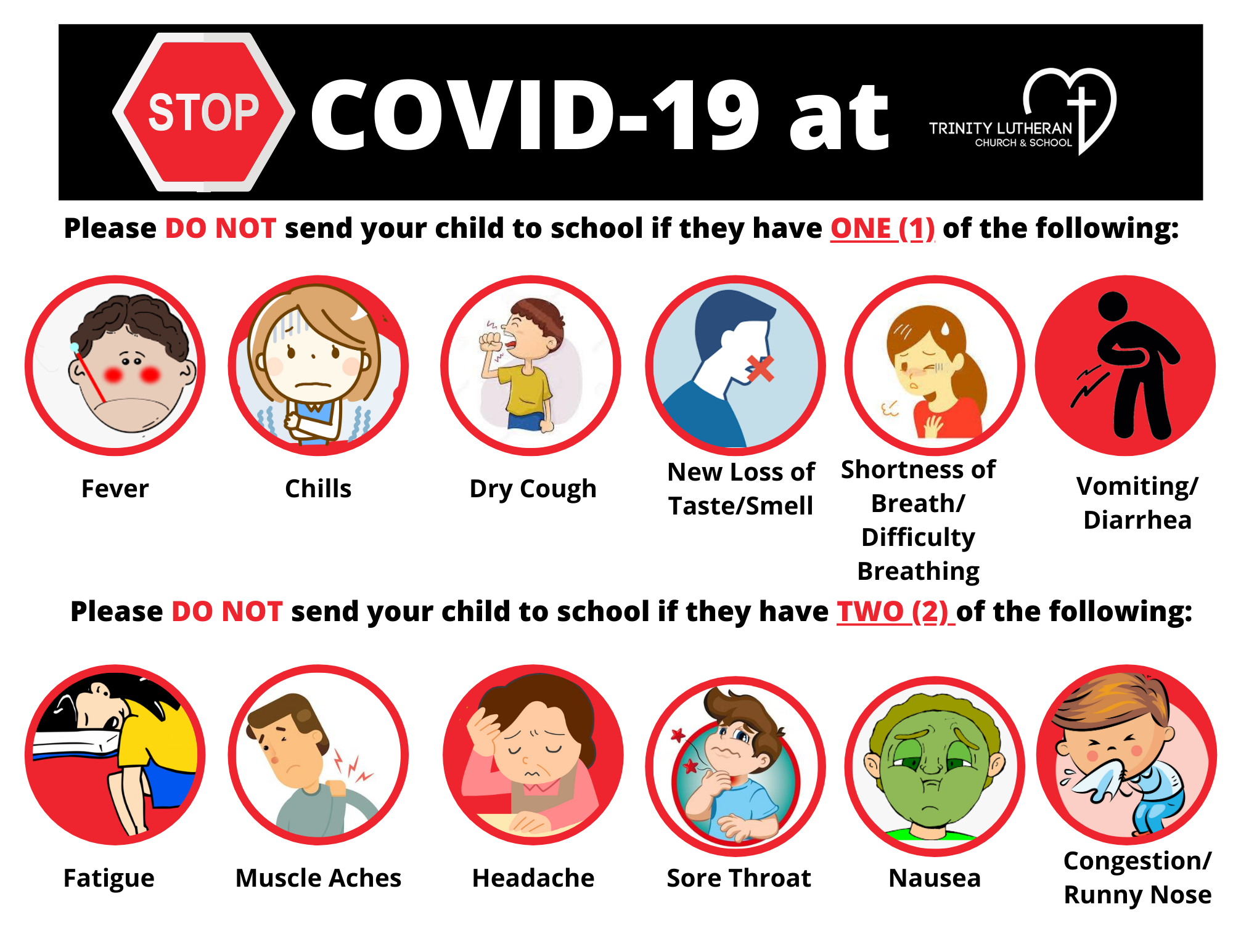
We need your help to stop COVID-19 at TLS. Please follow the screening tool below:
Does the child have any ONE of the following? (Single symptom list) – If yes, please do not send your child to school
O YES O NO FEVER
O YES O NO REPEATING SHAKING WITH CHILLS
O YES O NO DRY COUGH
O YES O NO NEW LOSS OF TASTE OR SMELL
O YES O NO SHORTNESS OF BREATH OF DIFFICULTY BREATHING
O YES O NO VOMITING
O YES O NO DIARRHEA
Does the child have TWO of the following? (Multiple symptom list) – If you, please do not send your child to school
O YES O NO FATIGUE
O YES O NO MUSCLE ACHES
O YES O NO HEADACHE
O YES O NO SORE THROAT
O YES O NO NAUSEA
O YES O NO CONGESTION OR RUNNY NOSE
Here is the full Family Health Screening Tool